

Mahesh Jayaraman: PGT-A Controversy Raises Questions on IVF Outcomes and Embryo Selection
Mahesh Jayaraman, Co-Founder of Sepalika, shared a post on LinkedIn:
“A popular IVF test is now being challenged in U.S. courts.
Not because it never works.
Not because everyone thinks it is useless.
But because some patients claim they were led to believe the test was more certain—and more beneficial—than the evidence actually supports.
The test is called PGT-A (Preimplantation Genetic Testing for Aneuploidy).
At first glance, the idea sounds obvious.
Test embryos for chromosome abnormalities.
Transfer the healthiest embryo.
Improve outcomes.
What’s not to like?
The controversy begins because PGT-A does not directly test the cells that become the baby.
Instead, it usually samples a small number of cells from the embryo’s outer layer (the trophectoderm), which primarily contributes to the placenta rather than the fetus itself.
And over the years, healthy babies have been born from some embryos that PGT-A classified as mosaic and, more rarely, from embryos initially considered abnormal.
This matters most for women who have very few embryos available. As a clinic that people come to after most else has failed, Sepalika sees more than its fair share of such patients.
If a potentially viable embryo is rejected, the consequences are not statistical.
They are personal.
But perhaps the most important question is this:
Does PGT-A increase the chance of taking home a baby?
Sometimes.
But not always.
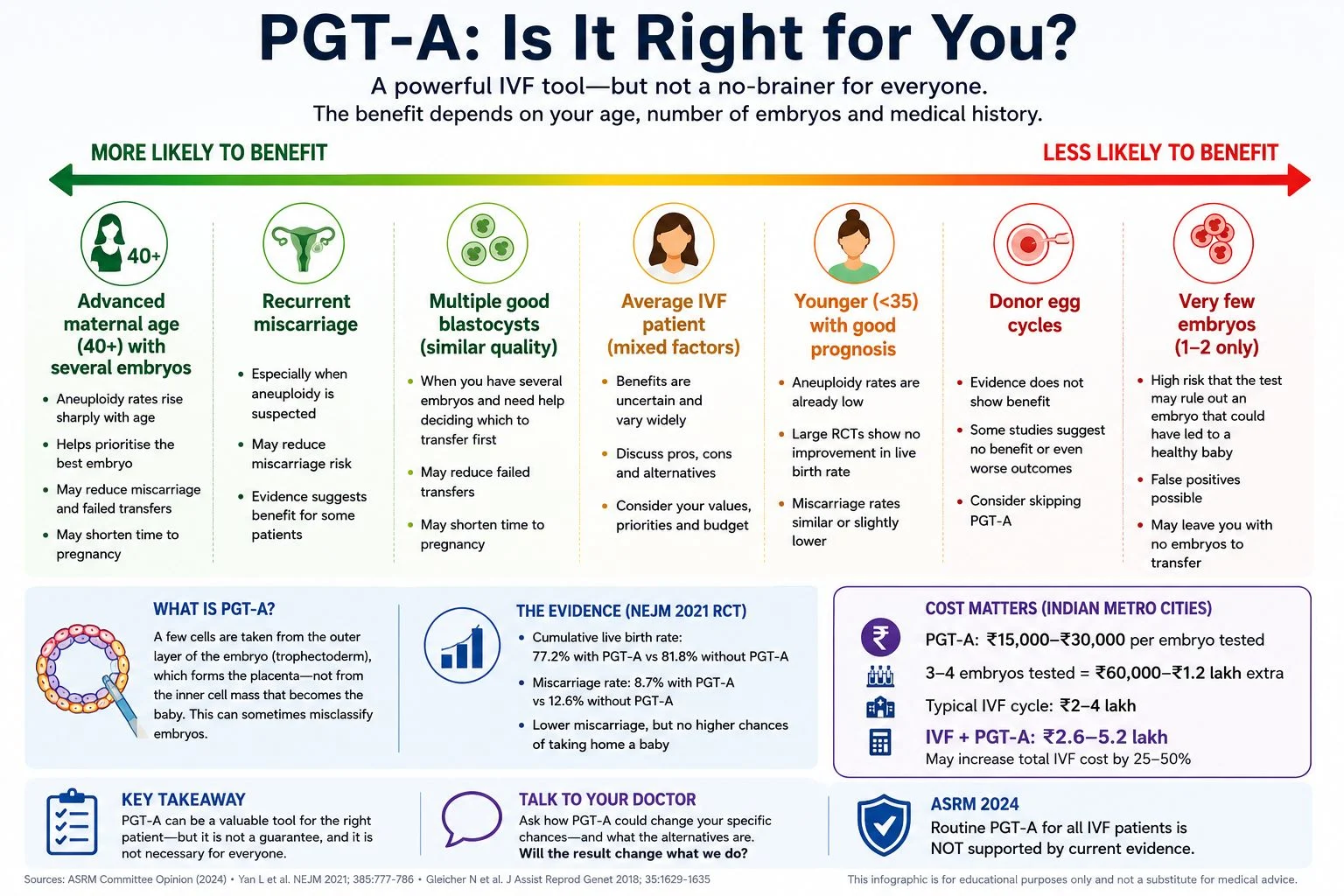
In a large 2021 randomized trial involving women aged 20–37 who had at least three good-quality blastocysts available, cumulative live birth rates were 77.2% with PGT-A and 81.8% without PGT-A, although miscarriage rates were lower with PGT-A.
This is one reason why the American Society for Reproductive Medicine (ASRM) concluded in 2024 that the value of PGT-A as a routine screening test for all IVF patients has not been demonstrated by current evidence.
And it isn’t cheap.
In India, PGT-A often adds roughly ₹50,000–₹1.5 lakh or more to an IVF cycle, depending on the clinic, laboratory, and number of embryos tested.
My take?
PGT-A is a tool.
A potentially useful one.
But not a universal no-brainer.
Its value depends heavily on age, embryo number, miscarriage history, prior IVF failures, laboratory quality, counselling, and how mosaic results are handled.
Of late, there have been posts suggesting that PGT-A is a test only fools would refuse in any IVF cycle.
The truth is more nuanced.
I’ve attached an infographic showing where PGT-A may be more useful, where benefit appears less clear, and why the debate remains so active.
(Design credit: ChatGPT)
For my IVF specialist colleagues:
- Which patient would you strongly recommend PGT-A for?
- And which patient would you advise to save the money?”
Stay updated on all scientific advances in the field of fertility with Fertility News.
-
Jul 25, 2026, 10:56PMOS Can Affect Much More Than Periods or Fertility – PCOS Awareness Association
-
Jul 25, 2026, 10:42Asma Khalil: Recreational Drug Use During Pregnancy, What Every Expectant Mother Should Know!
-
Jul 25, 2026, 10:40Khalil Faaed: Are Complex Y Chromosome Rearrangements the Missing Link in Unexplained Male Infertility?
-
Jul 25, 2026, 10:38Sean Lauber: Does Transferring a Cleavage or Blastocyst Stage Embryo Affect the Chance of Having a Boy?
-
Jul 25, 2026, 10:33Rokaya Hachicho: The Hidden Cost of Excessive Laser Use During Trophectoderm Biopsy!
-
Jul 25, 2026, 10:31Join the ISUOG Webinar on Late-Evolving Fetal Anomalies – ISUOG
-
Jul 25, 2026, 10:29Waiting Before Clamping the Umbilical Cord Improves Neonatal Outcomes! – RCOG
-
Jul 25, 2026, 10:27Christopher Robinson: The Impact of Body Mass Index on Misoprostol Dosing for Labor Induction!
-
Jul 25, 2026, 10:26Heavy Menstrual Bleeding and Dysmenorrhea in Adolescents – IJGO