

Shanza Ghaffar: Recurrent Pregnancy Loss Beyond Diagnosis and Treatment
Shanza Ghaffar, Reproductive Medicine Specialist/Gynecologist at Omar Hospital and Cardiac Centre, shared a post on LinkedIn:
“Recurrent Pregnancy Loss –
What Every Clinician (and Patient) Needs to Know
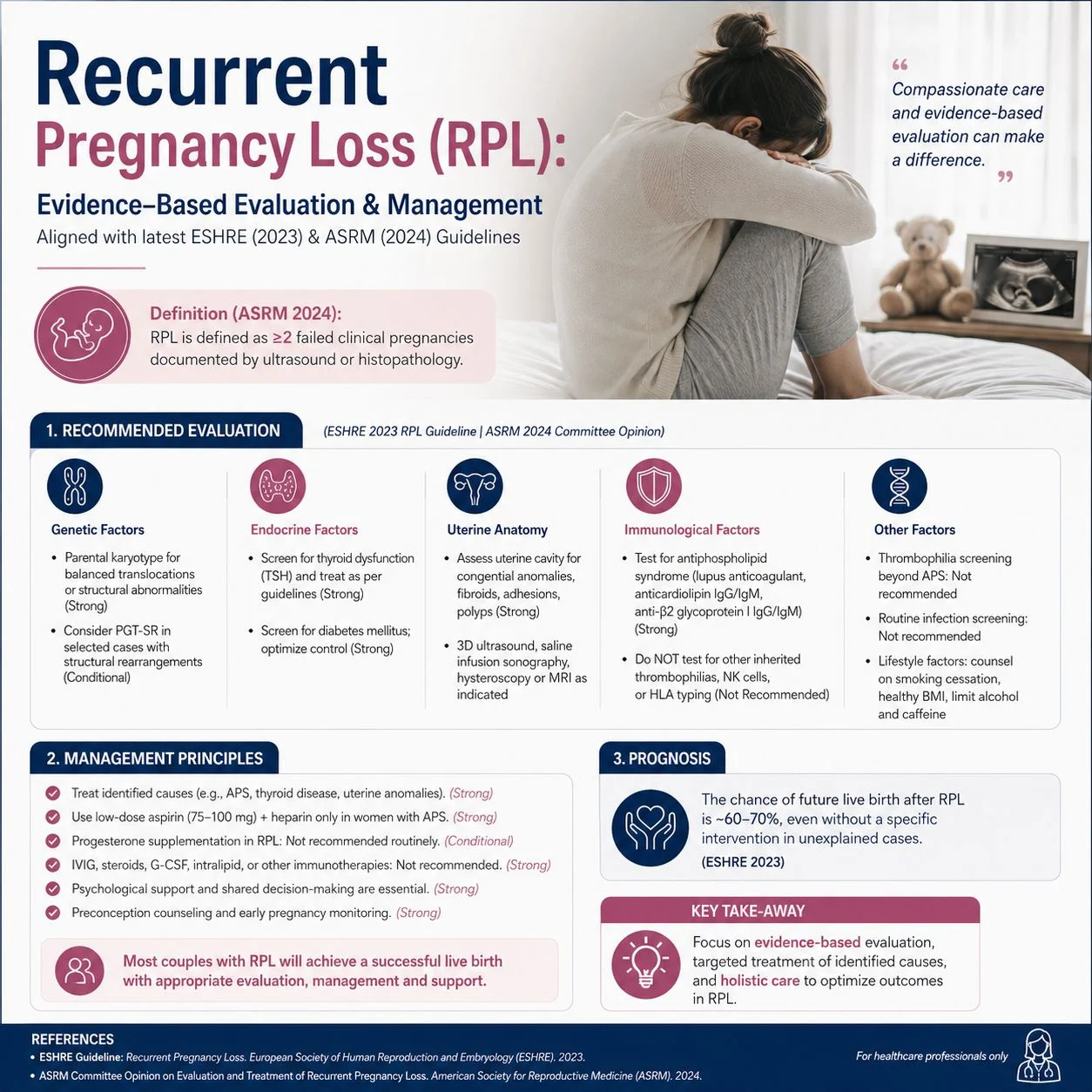
One miscarriage is devastating. Two or more? It shakes a person to their core. Recurrent Pregnancy Loss (RPL) affects 1–5% of couples trying to conceive, yet it remains one of the most underdiagnosed and emotionally under-supported conditions in reproductive medicine.
Here’s what the ESHRE and ASRM guidelines tell us:
Definition
Both ESHRE and ASRM now define RPL as 2 or more pregnancy losses before viability – and recommend starting investigations after just 2 losses. We no longer ask patients to wait for three.
Causes — and the humbling truth
We can only identify a cause in less than 50% of cases. Known causes include:
- Chromosomal / genetic factors (most common)
- Uterine anomalies — especially septate uterus
- Antiphospholipid Syndrome (APS)
- Thyroid dysfunction, diabetes, hyperprolactinemia
- Advanced maternal age
What we should do
- Screen for antiphospholipid antibodies (LA, aCL IgG/IgM) after 2 losses
- 3D ultrasound / hysteroscopy to rule out uterine anomalies
- Check TSH — target < 2.5 mIU/L, treat if elevated with anti-TPO positivity
- Parental karyotyping + POC chromosomal analysis
- For confirmed APS: low-dose aspirin pre-conception + LMWH once pregnancy confirmed
What we should not do routinely
- Routine inherited thrombophilia screening (Factor V Leiden etc.) — not recommended unless personal/family history of clots
- IVIg — no proven benefit
- Paternal leukocyte immunisation — trials show no improvement
- Routine NK cell testing — evidence remains insufficient
The most underrated intervention?
Tender Loving Care.
Both ESHRE and ASRM acknowledge that dedicated early pregnancy surveillance and emotional support are associated with improved live birth rates – even without pharmacological intervention. Compassionate care is not soft medicine. It is evidence-based medicine.
Progesterone?
May be considered in unexplained RPL, especially with early pregnancy bleeding (PRISM trial data). ASRM is more cautious – insufficient evidence for routine use, but widely used empirically given its safety profile.
RPL is not just a clinical problem. It is a grief that most people carry silently. As clinicians, our job is not only to investigate – it is to witness, to validate, and to walk alongside our patients with both scientific rigour and human warmth.
References:
ESHRE Guideline Group on RPL, Hum Reprod Open 2023 ·
ASRM Practice Committee, Fertil Steril 2024″
Stay updated on all scientific advances in the field of fertility with Fertility News.
-
Jul 13, 2026, 15:51Why Do We Need an Early Detection Test for Ovarian Cancer? – OCRF
-
Jul 13, 2026, 15:49Christopher Robinson: Internal Manual Aortic Compression for Temporary Control of Obstetric Pelvic Hemorrhage!
-
Jul 13, 2026, 15:46Can AI Reliably Predict IVF Outcomes? – Oasis Fertility
-
Jul 13, 2026, 15:44Marco Zaccaria: EndoLatam Brings Together Latin America’s Leaders in Endometriosis Care!
-
Jul 13, 2026, 15:21Jalid Sehouli: Please, Learn from the Past…and Fight for a Better Health Care System
-
Jul 13, 2026, 15:13This Week is Birth Trauma Awareness Week – Preeclampsia Foundation
-
Jul 13, 2026, 14:51World Population Day Reminds Us That Population Trends are About More Than Numbers – CFAS
-
Jul 13, 2026, 14:34Christopher Robinson: Predictive Value of Cervical Length Measured After 24 Weeks for Spontaneous Preterm Birth
-
Jul 13, 2026, 14:17Evelyn Ndinda: What are Purposes of the 20th and 24th Week Prenatal Visits?