

Rukmini Bezbaruah: Interpreting p53 Across Gynaecological Cancers
Rukmini Bezbaruah, Associate Professor Oncopathology at Dr. B. Borooah Cancer Institute, shared a post on LinkedIn:
“Interpreting p53 Across Gynaecological Cancers: One Marker, Multiple Meanings
In gynaecological pathology, TP53 is one of the most frequently altered genes. Yet, its immunohistochemical interpretation is often reduced to a simplistic label – ‘positive’ or ‘negative.’
That approach is no longer acceptable.
p53 must be interpreted as a pattern, and more importantly, in the context of tumour type.
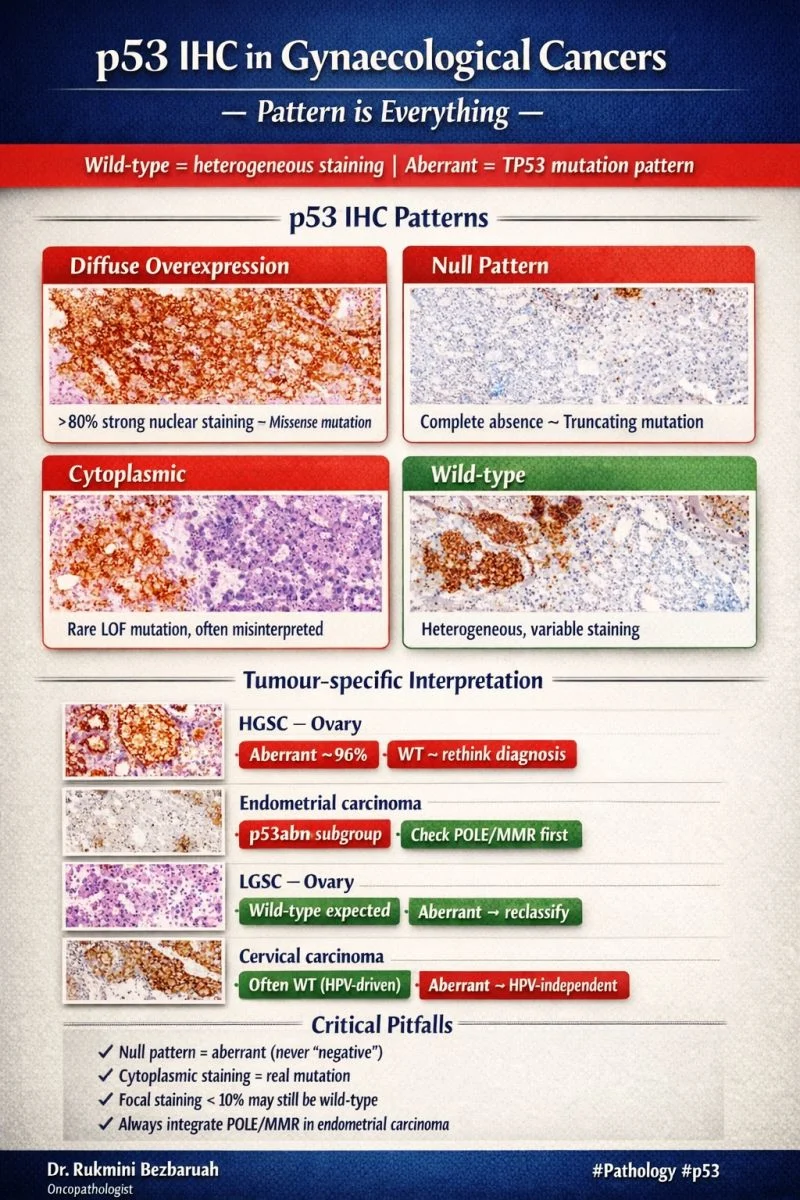
Core principle: Pattern-based interpretation
- Wild-type (p53wt) → patchy, variable nuclear staining
- Abnormal (p53abn) →
- Diffuse strong nuclear (overexpression)
- Complete absence (null)
- Cytoplasmic (rare)
- Subclonal (emerging category)
Tumour-specific interpretation matters
1. High-grade serous carcinoma (ovary/fallopian tube)
- Nearly universal p53 abnormality
- p53abn = diagnostic support
- p53wt → reconsider diagnosis
2. Endometrial carcinoma
- Majority are p53 wild-type
- p53abn defines a distinct molecular subgroup with poor prognosis
- Now integrated into molecular classification algorithms
3. Low-grade serous carcinoma
- Typically p53 wild-type
- p53abn → red flag for misclassification
4. Clear cell carcinoma
- Heterogeneous p53 expression
- Interpretation requires strong morphologic correlation
5. Cervical carcinoma
- p53 IHC is less reliable as a surrogate marker
- In HPV-associated tumors, p53 is often degraded → variable staining
What do recent guidelines emphasize?
- p53 is a surrogate for mutation, not a simple marker
- Interpretation must be:
- Pattern-based
- Context-specific
- Integrated with morphology and molecular data
- In endometrial carcinoma, p53 status is now part of:
- ESGO–ESTRO–ESP classification
- FIGO 2023 staging refinement
Common pitfalls
- Reporting ‘p53 positive’
- Missing null pattern due to lack of internal control
- Overcalling wild-type as abnormal
- Ignoring tumour context
Take-home message
p53 does not behave the same across all gynaecological cancers.
Its value lies not just in detection – but in interpretation within the right biological and morphological framework.”
Stay updated on all scientific advances in the field of fertility with Fertility News.
-
Jul 1, 2026, 16:01ASRM Launches Educational Podcast Series to Support LGBTQ+ Family-Building Journeys
-
Jul 1, 2026, 15:40Vakkanal Paily Awarded RCOG Distinguished Service Medal for Transforming Maternal Care in Kerala – RCOG
-
Jul 1, 2026, 15:11It All Comes Down to One Molecule – VEGF – Fertility Plus
-
Jul 1, 2026, 12:02Christopher Robinson: Impact of Maternal Aspirin Therapy on Neonatal Epigenetic Patterns
-
Jul 1, 2026, 11:25Could the Microbiome Help Improve Our Ability to Predict Pregnancy Complications – Reproduction and Fertility
-
Jul 1, 2026, 11:04Virtual PCOS CON 2026 to Bring Expert-Led Education to Patients Everywhere – PCOS Awareness Association
-
Jul 1, 2026, 10:38Progestin Analogues Effectively Restore FOXM1 Expression but Leave Key Gaps – RBMO
-
Jul 1, 2026, 10:24Dora Koller: Grouping Symptoms Across Body Systems Could Improve Endometriosis Diagnosis
-
Jul 1, 2026, 10:09Zofia Kiestrzyn: Award-Winning Research on Endometrial Cancer in Uterine Polyps