
Akansha Negi: AMH – A Number That Guides Treatment, Not a Number That Defines Fertility
Akansha Negi, Trainee Embryologist – Akanksha Ivf Centre at Mata Chanan Devi Hospital, shared a post on LinkedIn:
“AMH: A Number That Guides Treatment, Not a Number That Defines Fertility
‘Doctor, my AMH is 0.8. Does this mean I can never become pregnant?’
Perhaps no fertility marker creates as much anxiety or is as misunderstood as Anti-Müllerian Hormone (AMH).
AMH is not a fertility score. It estimates ovarian reserve – the number of follicles available to respond to stimulation, not egg quality or the ability to conceive.
Produced by the granulosa cells of pre-antral and small antral follicles (2–8 mm), AMH remains relatively stable throughout the menstrual cycle, making it a reliable marker of ovarian reserve.
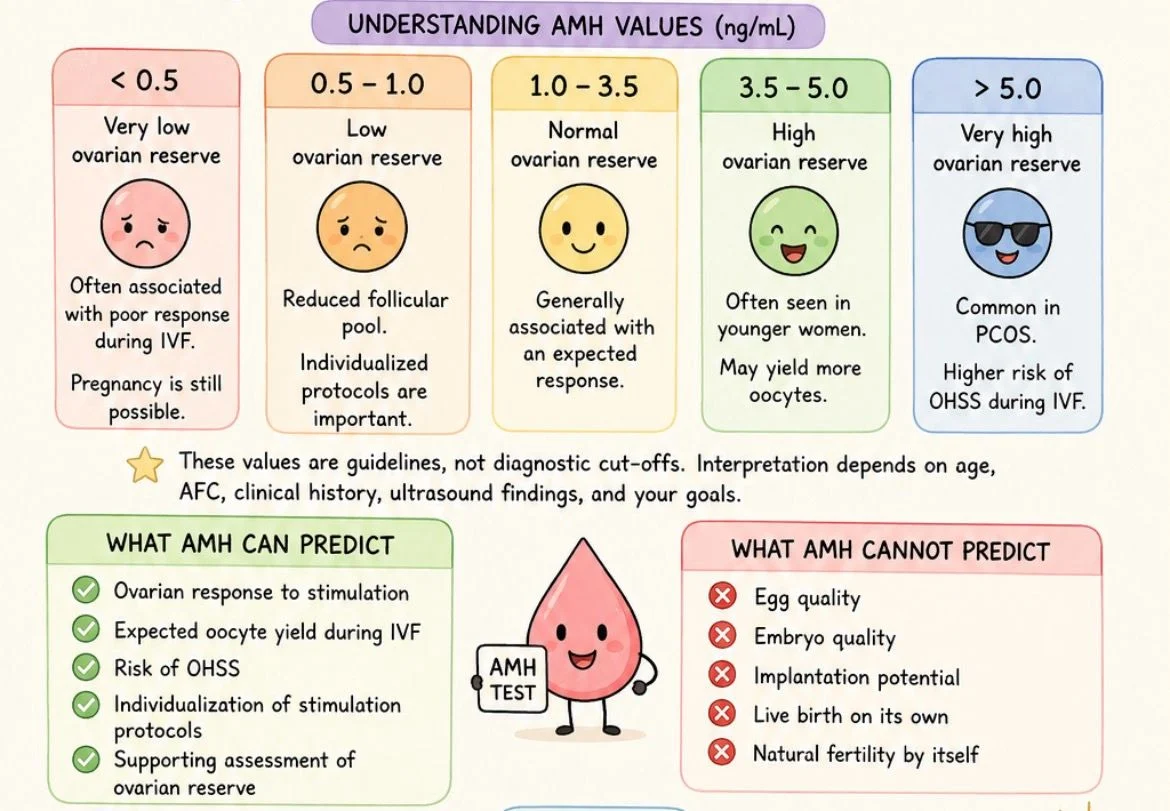
Understanding AMH values
- <0.5 ng/mL – Very low ovarian reserveOften associated with poor ovarian response during IVF.
Pregnancy is still possible, especially in younger women. - 0.5–1.0 ng/mL – Low ovarian reserveReduced follicular pool.
Individualized stimulation protocols are important. - 1.0–3.5 ng/mL – Normal ovarian reserveUsually associated with an expected response to ovarian stimulation.
- 3.5–5.0 ng/mL – High ovarian reserveOften seen in younger women.
May yield more oocytes. - >5.0 ng/mL – Very high AMHCommon in women with PCOS/PMOS
Increased risk of Ovarian Hyperstimulation Syndrome (OHSS) during IVF.
These values are guidelines not diagnostic cut-offs. Interpretation should always consider age, Antral Follicle Count (AFC), clinical history, and ultrasound findings.
What AMH predicts
- Ovarian response to stimulation
- Expected oocyte yield during IVF
- Risk of OHSS
- Individualization of stimulation protocols
What AMH cannot predict
- Egg quality
- Embryo quality
- Implantation potential
- Live birth on its own
- Natural fertility by itself
A 28-year-old with an AMH of 0.8 ng/mL may still have good-quality oocytes and conceive successfully.
A 40-year-old with an AMH of 3.0 ng/mL may retrieve more oocytes, but age-related decline in egg quality remains the greater challenge.
AMH predicts quantity. Age remains the strongest predictor of quality.
As embryologists, AMH should be viewed as a clinical compass not a final verdict. It should always be interpreted alongside age, AFC, endocrine profile, and clinical findings.
Numbers guide treatment. They should never define hope.
What is the most common misconception you’ve encountered about AMH?”
Stay updated on all scientific advances in the field of fertility with Fertility News.
-
Jun 23, 2026, 15:37Sergio Haimovich: A Septate Uterus Is Not Only a Fertility Issue But Also Influences Fetus Growth
-
Jun 23, 2026, 14:51UOG Journal Special Issue to Spotlight Advances in Congenital Heart Disease Research – ISUOG
-
Jun 23, 2026, 14:39Gynaecological Ultrasound Takes Centre Stage at Pre-ISUOG Educational Course – Gynaia
-
Jun 23, 2026, 12:39Christopher Robinson: The Pelosi Cesarean Delivery Technique – Pfannenstiel Incision
-
Jun 23, 2026, 12:36Harald Krentel: Stockholm Hosts Leading Experts in Robotic Gynecological Surgery
-
Jun 23, 2026, 11:36Fertility Strategy For Women with Polycystic Ovary Syndrome – IVF or IVM – MEFS
-
Jun 23, 2026, 11:22Contraceptive Strategies for Reducing the Risk of Reproductive Cancers – IJGO
-
Jun 23, 2026, 11:20Bringing C-RHI Back, A Story of Persistence and Professional Pride – ASRM
-
Jun 23, 2026, 10:56Christopher Robinson։ Avoiding Placental Transection During Cesarean Delivery for Anterior Placenta Previa